Is Energy Healing Just Placebo? The Real Answer

Some of energy healing's effect is placebo. The placebo effect is itself real and measurable, with documented mechanisms in pain modulation and autonomic regulation. The 2017 Baldwin Reiki RCT showed real-Reiki recipients had respiration drop that sham-Reiki did not match. The 2017 McManus systematic review concluded Reiki outperforms placebo on multiple measures. The most accurate framing is "the effect is partly placebo, partly autonomic regulation, partly therapeutic relationship, with the proportions varying by modality and condition."
Key Questions Answered
Is energy healing just the placebo effect?
No, but the placebo effect is real and accounts for part of what energy healing does. The Baldwin 2017 Reiki RCT and the McManus 2017 systematic review both found effects that exceeded sham conditions. The honest answer is "partly placebo, partly mechanism, partly relationship."
How much of the effect is placebo?
It varies by modality and condition. Some research suggests 30-50% of the total effect for some pain conditions is attributable to placebo. The remainder appears to come from autonomic regulation, the therapeutic relationship, and possibly modality-specific mechanisms.
Why does the placebo effect matter clinically if it is "just placebo"?
Because placebo effects are real biological events. Endogenous opioid release. Dopaminergic activation. Cortisol reduction. They reduce pain and anxiety in measurable ways. "Just placebo" is not nothing. It is a real treatment effect with real biology.
What is the difference between real Reiki and sham Reiki in studies?
In sham Reiki the practitioner mimics hand positions without intentional energy work. The 2017 Baldwin study at Cleveland Clinic compared real Reiki, sham Reiki, and standard care after total knee replacement. Real Reiki produced larger respiration rate reduction than sham Reiki. This suggests effect beyond pure placebo.
How can I tell if my own response is real or placebo?
Honestly, you cannot fully tell. And it does not matter clinically. The right test is whether you feel measurably better, function better, sleep better. Not whether the mechanism is placebo or not. Placebo response is real biology. Use what works for you.
In This Guide
Key Takeaways
- The placebo effect is itself a real, measurable biological phenomenon, with documented effects on pain, anxiety, and autonomic regulation.
- A 2024 American College of Physicians review of placebo effects in clinical practice noted significant impact on subjective symptoms and recommended ethical use as adjunct care.
- The 2017 Baldwin Reiki RCT compared real Reiki, sham Reiki, and standard care, finding real Reiki produced respiration drop that sham did not match.
- The 2017 McManus systematic review concluded Reiki outperforms placebo on pain, anxiety, depression, and self-esteem outcomes.
- The most accurate framing of energy healing effects is partly placebo, partly autonomic regulation, partly therapeutic relationship, with proportions varying by modality and condition.
Listen to the deep-dive on this article
A two-host audio overview of the key ideas. Origins, mechanism, evidence, and what to expect. Useful when you would rather listen than read.
Placebo Is Real Biology, Not Imagination
The first thing to clear up. The placebo effect is not "imagining you feel better." It is documented biology. Functional MRI studies show that placebo analgesia activates the same descending pain modulation pathways that opioid medications activate. Placebo administration produces measurable endogenous opioid release. Placebo response in Parkinson's disease produces dopaminergic activation in the striatum.
This means "it's just placebo" is not the dismissal it sounds like. It is "the patient's own neurochemistry produced a measurable treatment response triggered by the context of receiving care."
The American College of Physicians published a 2024 review of placebo effects in clinical practice, concluding that ethical use of placebo response is supported when patients are informed and the intervention is low-risk. Open-label placebos, where patients know they are taking inert pills, still produce significant effects on chronic pain and irritable bowel syndrome.
So when someone says energy healing is "just placebo," they are saying it triggers real treatment biology through context, expectation, and therapeutic relationship rather than through a unique mechanism. That is a real thing. It is not nothing.
How Much of the Effect Is Placebo
The honest answer varies by modality and condition. Pain studies with placebo arms suggest 30 to 50 percent of total treatment effect for chronic pain is attributable to placebo response across many interventions, not just energy healing. For acute pain the proportion is smaller. For anxiety the proportion is mid-range.
What this means in practice. If energy healing produces a 4-point drop on a 10-point pain scale, perhaps 1.5 to 2 points of that is placebo response. The remaining 2 to 2.5 points reflects mechanism beyond placebo (autonomic regulation, therapeutic relationship, possibly modality-specific effect).
The proportion is not a flaw. Placebo response is part of every intervention that involves human attention, ritual, and expectation. Surgical placebo studies show that sham knee surgery produces 60 to 70 percent of the pain relief of real knee surgery for some conditions. This does not invalidate real surgery. It contextualises it.
Every treatment that works through human contact has placebo as part of its mechanism. The relevant question is not "is there placebo?" The relevant question is "is the total effect clinically useful, at acceptable cost and risk?"
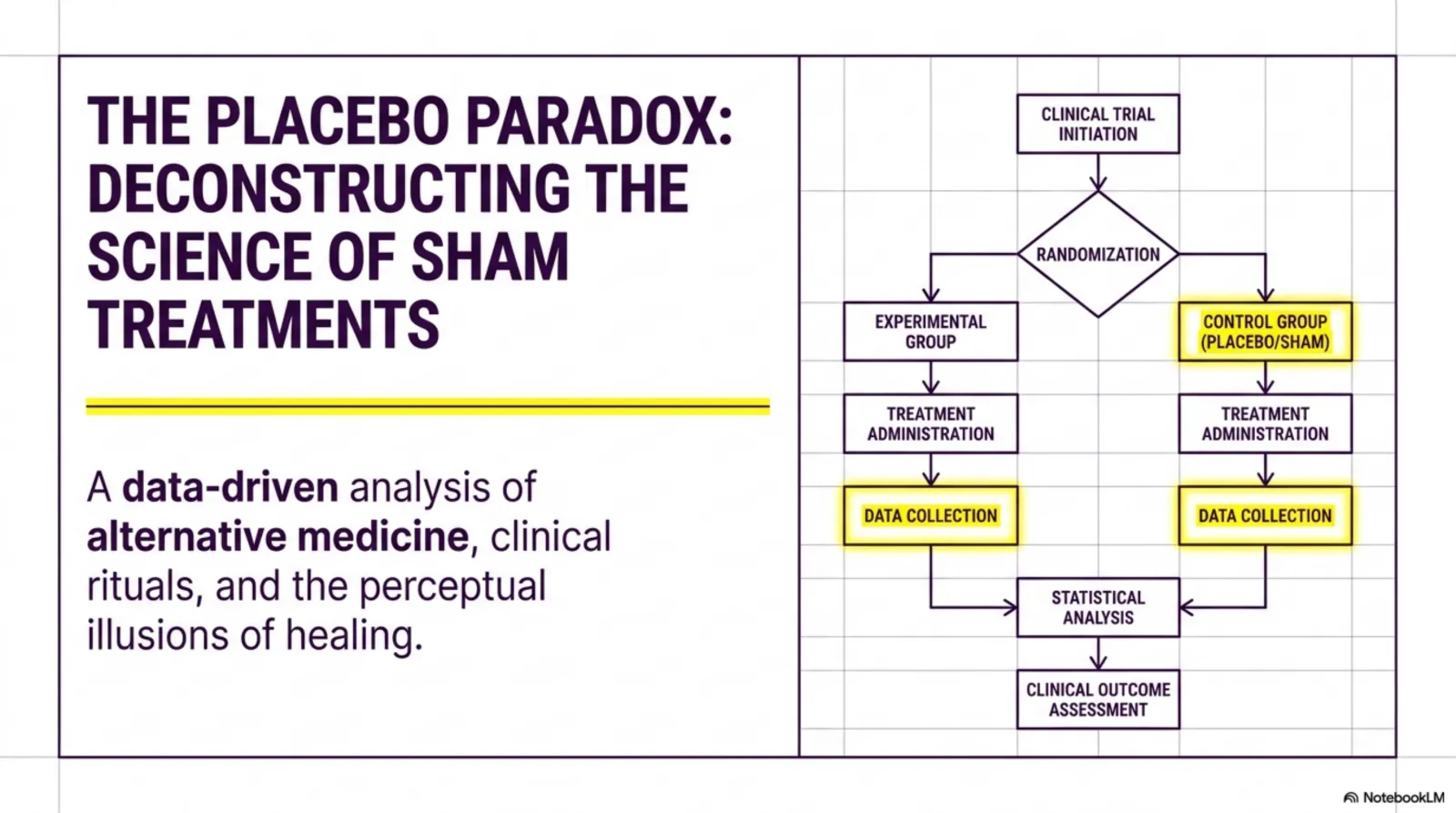
Real Versus Sham: What the Trials Show
The studies that try hardest to isolate non-placebo effect compare real treatment with carefully matched sham. In Reiki sham studies, the sham practitioner mimics hand positions and time on body without intentional energy work.
The 2017 Baldwin pilot at Cleveland Clinic ran this comparison after total knee replacement. The three arms were real Reiki, sham Reiki, and standard care. Real Reiki recipients showed greater respiration rate reduction at 48 hours (20.1 to 17.7 breaths per minute) than either sham Reiki or standard care alone.
This pattern, real producing more than sham, has appeared across several biofield trials. The differences are typically smaller than the differences between any active intervention and no-treatment controls. They are real and consistent enough to be unlikely from chance alone.
The 2017 McManus systematic review pulled together Reiki RCTs and concluded Reiki produces effects beyond placebo on multiple outcomes. The 2024 BMC Palliative Care Reiki meta-analysis covering 13 studies and 824 patients found significant anxiety reduction with effects strongest for short-term protocols.
None of this is large effect size. It is moderate effect with real signal above placebo. That is the honest reading of the strongest evidence in the field.
Where the Therapeutic Relationship Fits
Some of what energy healing does is the relationship. The hour of focused attention. The structured contact. The slowed pace. The non-judgmental presence.
Studies across all forms of medicine confirm this matters. Patients with stronger therapeutic alliances have better outcomes in psychotherapy, physical therapy, primary care, and complementary medicine. The therapeutic alliance contributes 5 to 15 percent of total outcome variance in psychotherapy meta-analyses.
For energy healing specifically, the relationship effect is large because the modality structure prioritises attention, presence, and slowed pace. A 60-minute Reiki session is structurally different from a 12-minute primary care visit. The relationship-mediated effects compound the modality-specific effects.
This is not a criticism. It is observation. If you are choosing between an honest energy healing practitioner who provides 60 minutes of structured attention and an exploitative consciousness coach who promises miraculous transformation, the relationship-mediated benefit favours the honest practitioner regardless of modality specifics.
Use practitioners who do this part well. The relationship-mediated effects are durable across many modalities. The modality-specific effects are smaller and contested.
When the Placebo Question Actually Matters
For symptom-management uses, the placebo question matters less than the cost and risk question.
Mild-to-moderate anxiety, chronic pain, post-surgical recovery, fatigue, sleep disruption. Energy healing produces moderate reliable benefit at low cost and minimal risk. Whether the mechanism is placebo, relationship, autonomic regulation, or all three, the pragmatic answer is the same. It is worth trying as adjunct care.
For primary disease treatment uses, the placebo question matters enormously. Cancer treatment, severe mental illness, autoimmune disease management. Here the requirement is not symptom relief but disease modification. Placebo and relationship effects do not modify cancer progression in any clinically meaningful way. Choosing energy healing in place of evidence-based treatment for serious disease is a serious mistake.
The honest practitioner navigates this distinction explicitly. They offer their work as adjunct care for symptoms. They do not claim disease modification.
The dishonest practitioner, or the well-meaning practitioner who has lost their evidence orientation, offers their work as primary treatment for serious disease. This is where the placebo question becomes ethically loaded. Real treatment biology is real. Disease modification is a different bar.
What This Means for Your Decision
Three frames are useful when deciding whether to try energy healing.
First. The effect is partly placebo. That is real biology, not nothing. If you respond to placebo, you respond. Your response is biologically valid.
Second. The effect is partly relationship. Choose practitioners who do the relationship part well. Slowed pace, focused attention, non-judgmental presence, honest scoping of what the work does and does not do.
Third. The effect may be partly modality-specific. The strongest studies suggest real-Reiki produces effects above sham-Reiki. The effect is moderate, not large. If your condition fits the evidence base for the modality, the modality-specific effect adds to the placebo and relationship effects.
Combined, these three layers produce moderate reliable benefit for symptom management at low cost and minimal risk. That is the realistic ceiling. Most people seeking energy healing for the conditions where the evidence is strong (anxiety, chronic pain, procedural distress, stress-related symptoms) will get useful relief.
Most people seeking energy healing for the conditions where the evidence is weak (cancer treatment, severe mental illness, structural disease) will not. Use the modality where the evidence supports it. Use other modalities where it does not.
Frequently Asked Questions
Why do critics say it is "just placebo" if research shows otherwise?
Because the methodological quality of the studies is limited, and "just placebo" is a defensible interpretation if you weight the limitations heavily. The Baldwin 2017 and McManus 2017 results do show effects above sham, but the studies are small, the blinding is imperfect, and the field as a whole has not produced a single definitive trial.
Are placebo effects ethical to use in clinical practice?
A 2024 American College of Physicians review concluded that ethical use of placebo response in clinical care is supported when patients are informed and the intervention is low-risk. Open-label placebos (where patients know they are taking inert pills) still produce measurable effects.
Does the therapeutic relationship matter?
Substantially. Studies of CBT, physical therapy, acupuncture, and energy healing all show that practitioner warmth, presence, and structured attention contribute meaningfully to outcomes. This is not a flaw in the research. It is part of how all human treatment works.
If it is partly placebo and partly mechanism, why not just call it placebo?
Because that erases the parts that are not placebo. The autonomic regulation effects are documented and measurable. The therapeutic-relationship effects are documented across all forms of medicine. The modality-specific effects (real Reiki versus sham Reiki) are smaller but consistent in the strongest studies.
Should I tell a practitioner I am skeptical?
Yes. The honest practitioners welcome it. They will not push beyond what the evidence supports. They will work with you within the realistic frame. The placebo response is not eliminated by skepticism; it is simply more modest.
Continue Reading
More from the blog
Keep exploring
Browse the rest of NeuralFlow's long-form guides on consciousness coaching, energy healing, and mind-body science. Every article is research-backed and built as a multi-format knowledge hub.
Read more articles